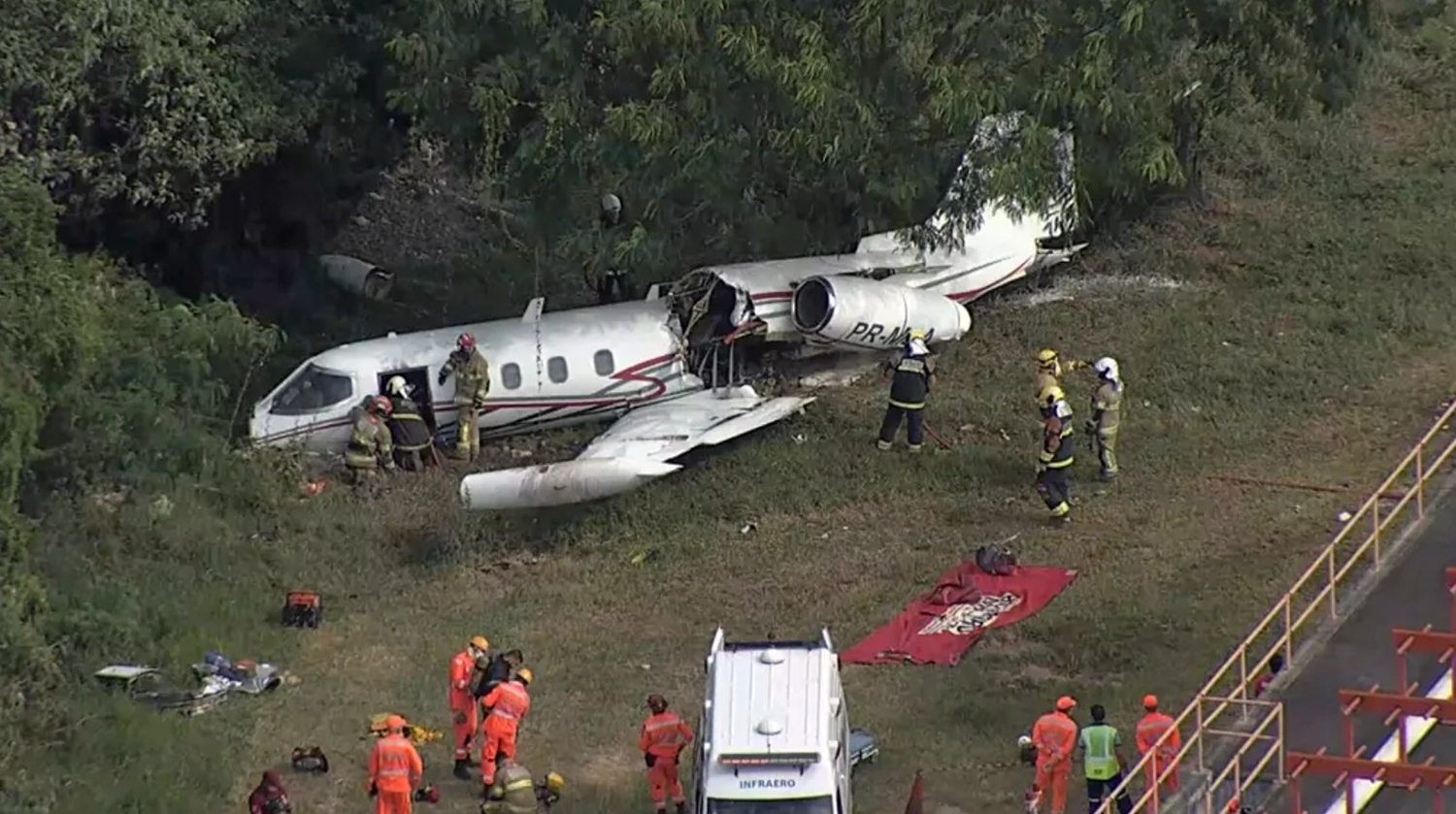
Crash of a Learjet 35A in Belo Horizonte: 1 killed
Date & Time:
Apr 20, 2021 at 1452 LT
Registration:
PR-MLA
Survivors:
Yes
Schedule:
Belo Horizonte - Belo Horizonte
MSN:
35-072
YOM:
1976
Crew on board:
2
Crew fatalities:
Pax on board:
1
Pax fatalities:
Other fatalities:
Total fatalities:
1
Captain / Total hours on type:
41.00
Copilot / Total hours on type:
2211
Circumstances:
The airplane departed Belo Horizonte-Pampulha-Carlos Drummond de Andrade Airport at 1420LT on a local training fight. On board were two pilots and one passenger. After 30 minutes of flight over the area, the crew returned to the airport and initiated the approach to runway 13 to complete a touch and go manoeuvre. On final approach, the crew forgot to lower the gear, causing the airplane to land on its belly. It slid for few hundred metres, overran, went through the perimeter fence (striking concrete poles) and came to rest against trees, broken in two. The copilot aged 76 was killed while both other occupants were injured.
Probable cause:
Contributing factors:
- Attention – undetermined.
It is possible that the aircraft’s encounter with a kite led to a delayed and imprecise response to operational cues, which may have resulted in a breakdown in the alert and distraction management system, specifically regarding landing gear extension.
- Attitude – undetermined.
Conducting the flight with an unqualified pilot reflected the adoption of inappropriate attitudes such as complacency, overconfidence, and disregard for the requirements established in RBACs 91 and 61, which may have contributed to this accident.
- Crew Resource Management – a contributor.
Inefficient use of the human resources available for the aircraft operation led to inadequate task management among the crew. The PIC never questioned the aircraft’s readiness for landing, and the pilot occupying the right seat failed to monitor the aircraft configuration or assertively advise on the landing gear position for touchdown.
- Perception – a contributor.
During the approach, the aural warning indicating that the landing gear was still retracted was activated and could be heard on the CVR audio. However, the pilots took no corrective action, evidencing impaired ability to recognize and interpret internal environmental cues, which led to reduced situational awareness and culminated in a gear up landing.
- Limited pilot’s experience – undetermined.
Considering the PIC’s operational background, developed almost entirely in rotary wing aviation, it is possible that his limited experience with fixed-wing aircraft had not yet enabled him to acquire the full range of skills and knowledge necessary for the safe operation of Learjet 35 flights.
- Attention – undetermined.
It is possible that the aircraft’s encounter with a kite led to a delayed and imprecise response to operational cues, which may have resulted in a breakdown in the alert and distraction management system, specifically regarding landing gear extension.
- Attitude – undetermined.
Conducting the flight with an unqualified pilot reflected the adoption of inappropriate attitudes such as complacency, overconfidence, and disregard for the requirements established in RBACs 91 and 61, which may have contributed to this accident.
- Crew Resource Management – a contributor.
Inefficient use of the human resources available for the aircraft operation led to inadequate task management among the crew. The PIC never questioned the aircraft’s readiness for landing, and the pilot occupying the right seat failed to monitor the aircraft configuration or assertively advise on the landing gear position for touchdown.
- Perception – a contributor.
During the approach, the aural warning indicating that the landing gear was still retracted was activated and could be heard on the CVR audio. However, the pilots took no corrective action, evidencing impaired ability to recognize and interpret internal environmental cues, which led to reduced situational awareness and culminated in a gear up landing.
- Limited pilot’s experience – undetermined.
Considering the PIC’s operational background, developed almost entirely in rotary wing aviation, it is possible that his limited experience with fixed-wing aircraft had not yet enabled him to acquire the full range of skills and knowledge necessary for the safe operation of Learjet 35 flights.
Final Report: