Crash of a Piper PA-31-350 Navajo Chieftain in Bangkok: 1 killed
Date & Time:
Aug 1, 2016 at 1605 LT
Operator:

Registration:
HS-FGB
Survivors:
Yes
Schedule:
Nakhon Ratchasima – Bangkok
MSN:
31-7652156
YOM:
1976
Flight number:
TRB106
Crew on board:
2
Crew fatalities:
Pax on board:
2
Pax fatalities:
Other fatalities:
Total fatalities:
1
Circumstances:
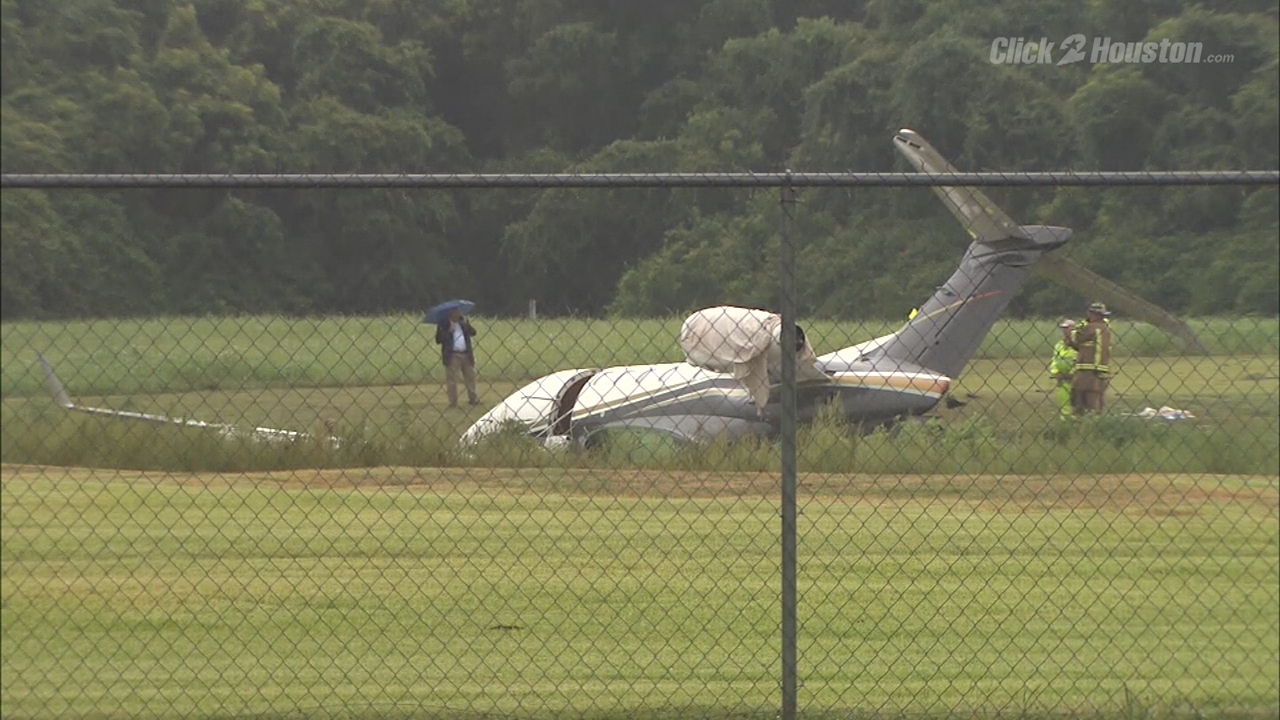
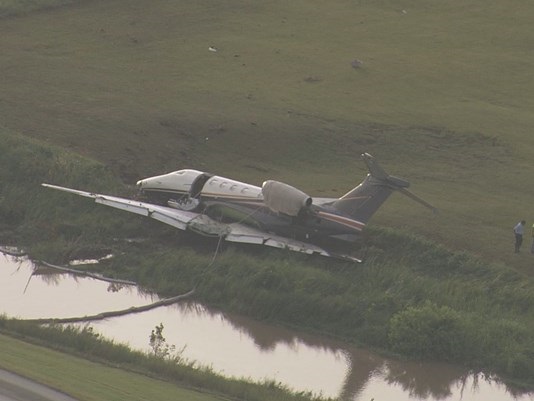
While descending to Bangkok-Suvarnabhumi Airport, the twin engine aircraft crashed in unknown circumstances in a swamp and came to rest against a wood bridge. The wreckage was found about 15 km from the airport, along the borders of Nong Chok and Min Buri districts. The captain was killed while three other occupants were injured.