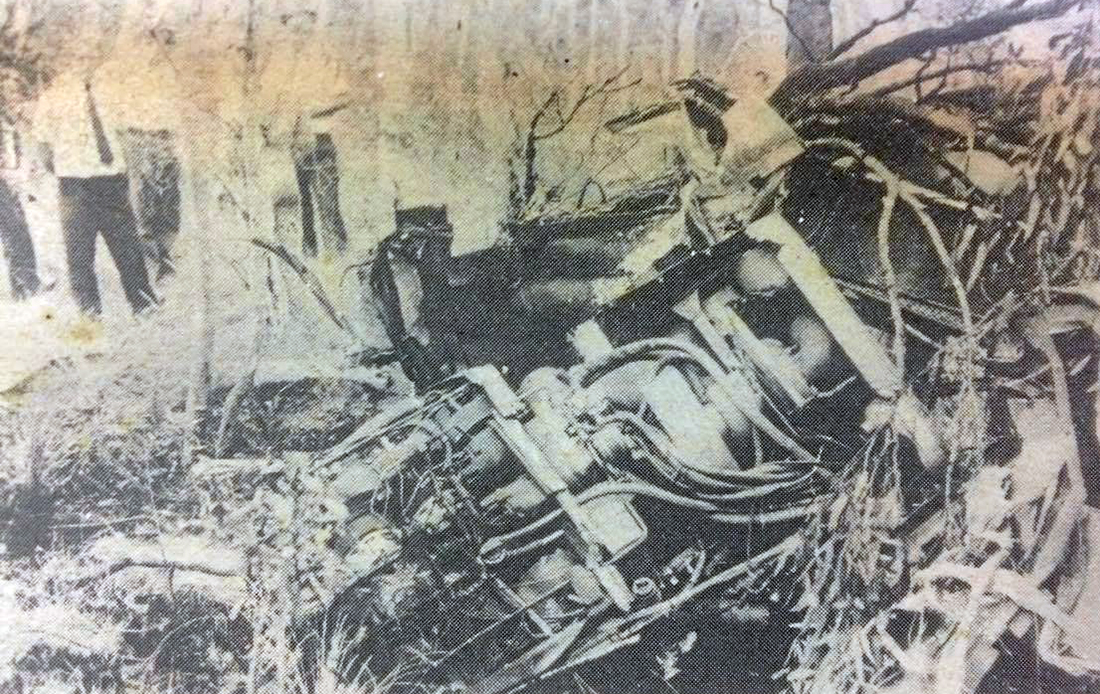
Crash of a Beechcraft A100 King Air in Chapleau: 4 killed
Date & Time:
Nov 29, 1988 at 2301 LT
Operator:

Registration:
C-GJUL
Survivors:
No
Schedule:
Timmins - Chapleau
MSN:
B-218
YOM:
1975
Flight number:
VC796
Crew on board:
2
Crew fatalities:
Pax on board:
2
Pax fatalities:
Other fatalities:
Total fatalities:
4
Aircraft flight hours:
9420
Circumstances:
The twin engine aircraft was dispatched from Timmins to Chapleau on an ambulance flight, carrying two medical staffs and two pilots. A patient should be boarded in Chapleau and transferred to Sault Sainte Marie. Following an uneventful flight at FL120, the crew started a night descent to Chapleau. On a final NDB approach, the aircraft struck the ground and crashed 2,5 km southwest of the airport. The aircraft was destroyed and all four occupants were killed.
Probable cause:
The flight crew descended below the minimum applicable IFR altitude while approaching the Chapleau NDB. It could not be determined why the crew allowed the aircraft to descend, in controlled flight, into the ground.