Crash of a Cessna 421C Golden Eagle III in Steamboat Springs: 2 killed
Date & Time:
Jun 17, 2024 at 1623 LT
Registration:
N245T
Survivors:
No
Schedule:
Longmont - Ogden
MSN:
421C-1104
YOM:
1981
Crew on board:
1
Crew fatalities:
Pax on board:
1
Pax fatalities:
Other fatalities:
Total fatalities:
2
Captain / Total hours on type:
59.00
Aircraft flight hours:
3139
Circumstances:
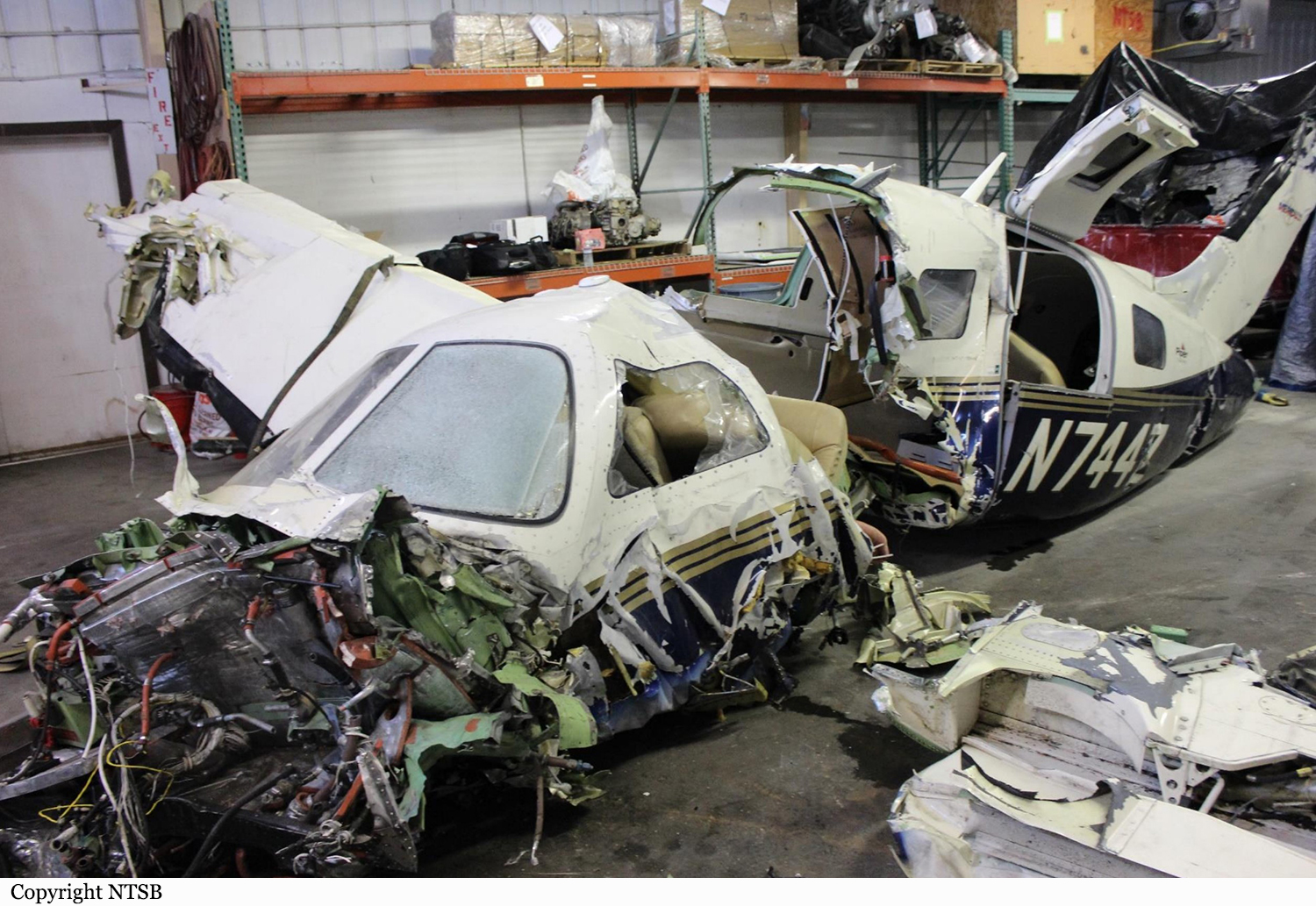
While enroute to the destination airport, the pilot reported a “cylinder temperature issue” to air traffic control (ATC) and the pilot diverted to another airport for a visual approach. The pilot overflew the airport and requested vectors for another visual approach. He then requested vectors to divert to an airport to the east before he informed air traffic control that the left engine lost power, and he received vectors back to the airport for a visual approach. The pilot maneuvered the airplane to land on runway 14, but for an unknown reason he decided to land on runway 32 instead. A pilot-rated witness reported that he observed the airplane while it was on the base to final turn for runway 32. He reported that the airplane’s wings leveled momentarily before it made a 60° left-bank turn and then entered a stall/spin in a counterclockwise rotation. The airplane impacted a trailer park about 0.38 miles from the approach end of runway 32. A postimpact fire ensued and destroyed the airplane. Examination of the airframe, flight controls, and the right engine did not detect any preimpact anomalies that would have precluded normal operation. Examination of the left engine found that the starter adapter spline was worn, with broken teeth on its crankshaft gear. The crankshaft gear remained properly timed with the crankshaft cluster gear, the investigation could not determine if the idler gear, which drives the magnetos, slipped timing. Mistiming of the magnetos could result in abnormal cylinder head temperature(s). In addition, there was improper hardware securing the cylinder No. 6 intake valve, which might have altered performance of that valve. Due to thermal damage, testing of the ignition and fuel systems could not be accomplished. Evidence of detonation was observed on the left engine’s piston heads. The installed engine data monitor was destroyed by the postimpact fire and did not provide further details as to the operational condition of the engine before the accident. Inspection of the starter adapter assembly is required annually by airworthiness directive and was accomplished on the most recent annual inspection. The airplane had flown about 5.5 hours since the inspection.
Probable cause:
The pilot’s failure to maintain sufficient airspeed following a loss of engine power, which resulted in an inadvertent aerodynamic stall/spin at low altitude.
Final Report: