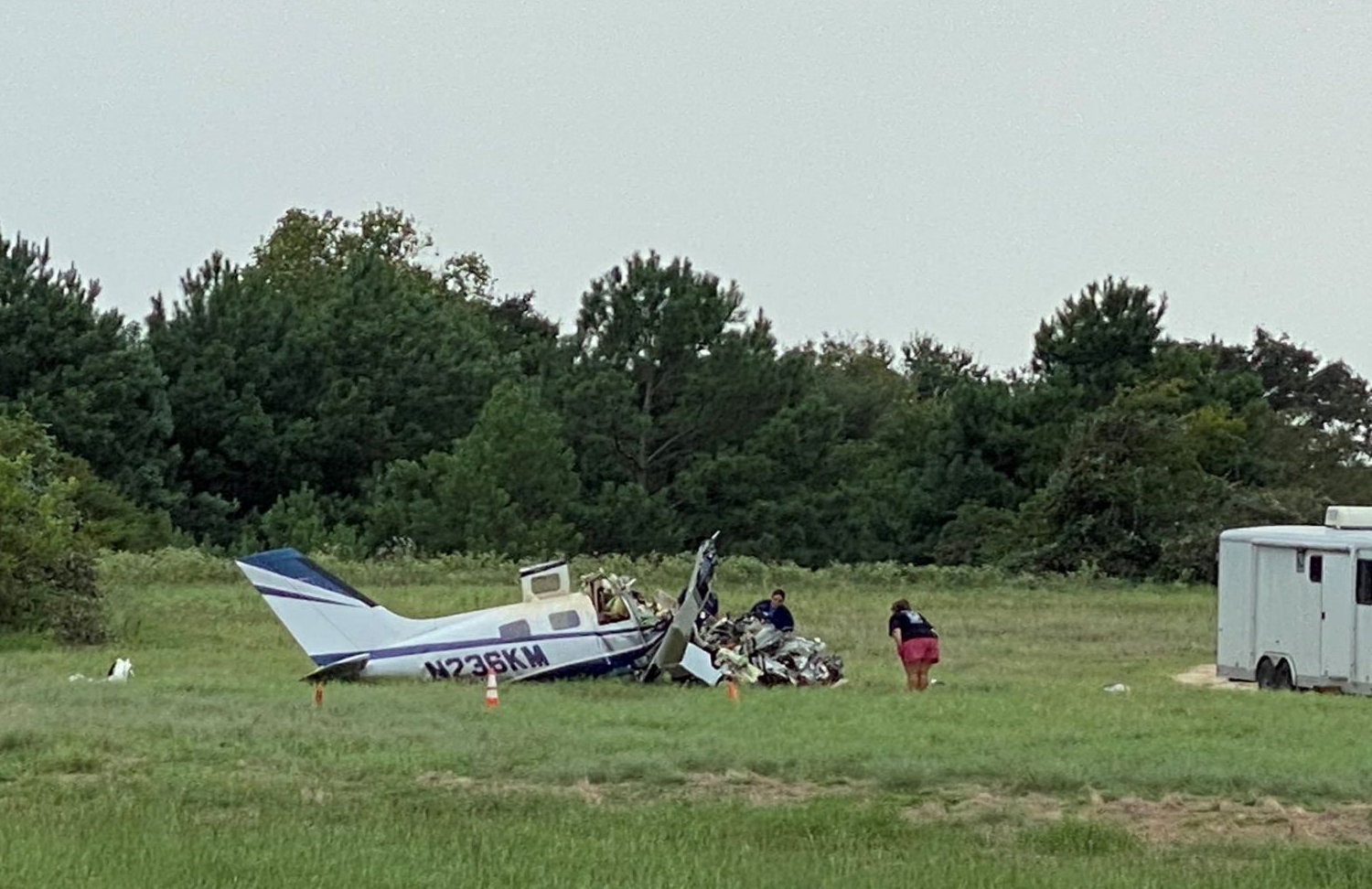
Crash of a Cessna 421C Golden Eagle III in Houston
Date & Time:
May 6, 2022 at 1418 LT
Operator:

Registration:
XB-FQS
Survivors:
Yes
Schedule:
Houston – San Antonio
MSN:
421C-0085
YOM:
1976
Crew on board:
1
Crew fatalities:
Pax on board:
3
Pax fatalities:
Other fatalities:
Total fatalities:
0
Captain / Total hours on type:
951.00
Aircraft flight hours:
5197
Circumstances:
The pilot reported that, before the flight, the airplane was fueled with 140 gallons of Jet A fuel. Shortly after takeoff, both engines lost total power. Because the airplane had insufficient altitude to return to the airport, the pilot executed a forced landing to a field and the left wing sustained substantial damage. A postcrash fire ensued. The investigation determined that the airplane was inadvertently fueled with Jet A fuel rather than AVGAS, which was required for the airplane’s reciprocating engines. The line service worker who fueled the airplane reported that there were no decals at the airplane fuel ports; however, postaccident examination of the airplane found that a decal specifying AVGAS was present at the right-wing fuel port. The investigation could not determine whether the same or a similar decal was present at the left-wing fuel port because the left wing was partially consumed during the postimpact fire.
Probable cause:
The fixed-base operator’s incorrect fueling of the airplane, which resulted in a total loss of power in both engines.
Final Report: