Crash of a Piper PA-46-350P Malibu Mirage in Parma: 3 killed
Date & Time:
Apr 23, 2008 at 1710 LT
Operator:

Registration:
D-EPOE
Survivors:
No
Schedule:
Parma - Parma
MSN:
46-22180
YOM:
1995
Crew on board:
2
Crew fatalities:
Pax on board:
1
Pax fatalities:
Other fatalities:
Total fatalities:
3
Aircraft flight hours:
1434
Circumstances:
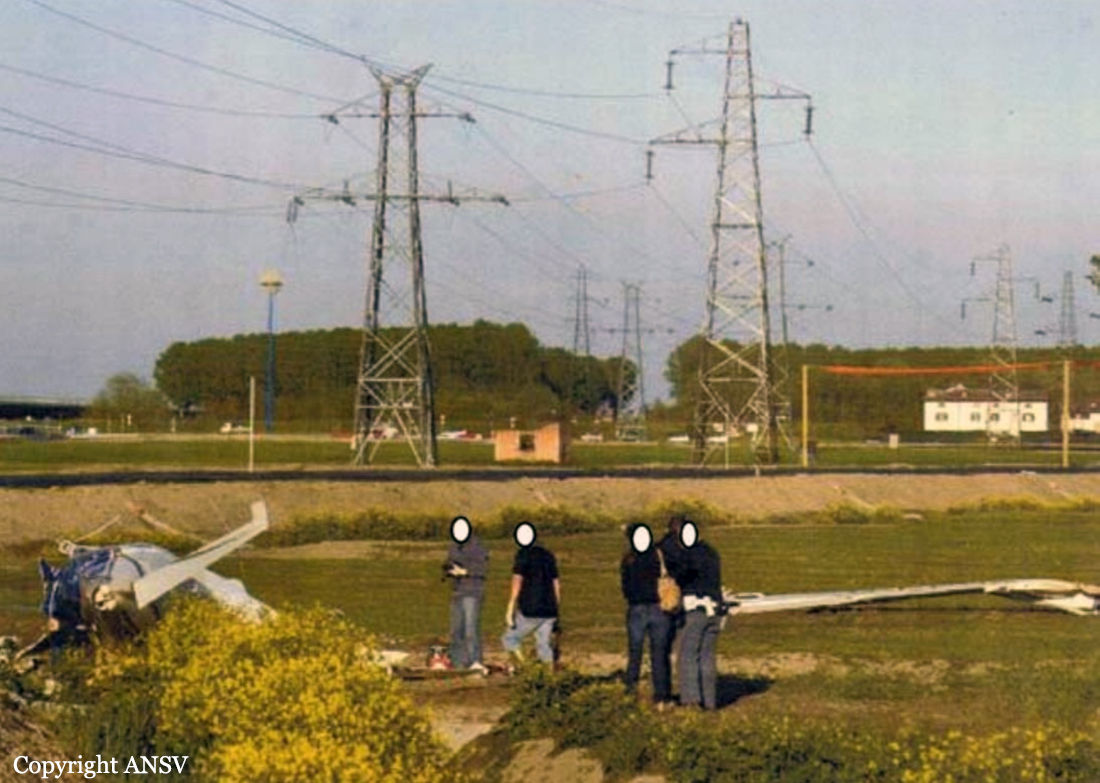
The single engine aircraft departed Parma-Giuseppe Verdi Airport at 1635LT on a local training flight, carrying one passenger (a PA-46 rated pilot), a pilot under supervision and one instructor. The goal of the flight was to revalidate the PA-46 licence of the pilot-in-command. Following a successful emergency landing and a touch-and-go, the crew followed a new circuit and was cleared for a new approach to runway 20 in VFR conditions. On short final, while completing a left turn to join the approach path, the aircraft stalled, collided with power lines and crashed near a roundabout located about 1,100 metres short of runway 20. The aircraft was destroyed and all three occupants were killed.
Probable cause:
A loss of control as a result of an aerodynamic stall while completing a left turn due to an insufficient speed. During the last turn facing the setting sun, the pilot-in-command reduced the engine power excessively, possibly after suffering a loss of situational awareness. The short distance between the aircraft and the ground did not allow the crew to expect a stall recovery.
Final Report: