Circumstances:
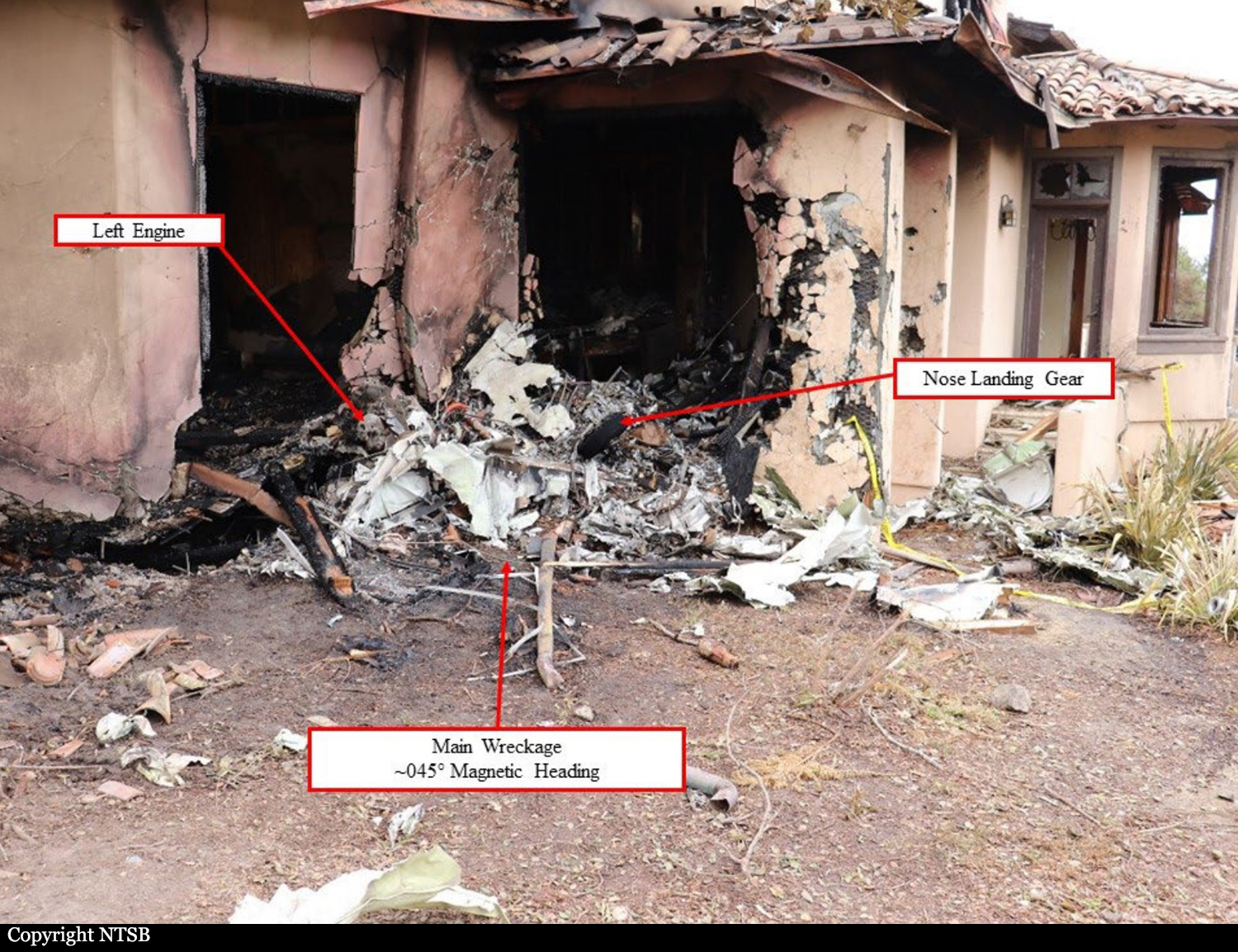
The flight crew was conducting a personal flight with two passengers onboard. Before departure, the cockpit voice recorder (CVR) captured the pilots verbalizing items from the before takeoff checklist, but there was no challenge response for the taxi, before takeoff, or takeoff checklists. Further, no crew briefing was performed and neither pilot mentioned releasing the parking brake. The left seat pilot, who was the pilot flying (PF) and pilot-in-command (PIC), initiated takeoff from the slightly upsloping 3,665-ft-long asphalt runway. According to takeoff performance data that day and takeoff performance models, the airplane had adequate performance capability to take off from that runway. Flight data recorder (FDR) data indicated each thrust lever angle was set and remained at 65° while the engines were set and remained at 91% N1. During the takeoff roll, the CVR recorded the copilot, who was the pilot monitoring (PM) and second-in-command (SIC), making callouts for “airspeed’s alive,” “eighty knots cross check,” “v one,” and “rotate.” A comparison of FDR data from the accident flight with the previous two takeoffs showed that the airplane did not become airborne at the usual location along the runway, and the longitudinal acceleration was about 33% less. At the time of the rotate callout, the airspeed was about 104 knots calibrated airspeed, and the elevator was about +9° airplane nose up (ANU). Three seconds after the rotate callout, the CVR recorded the sound of physical straining, suggesting the pilot was likely attempting to rotate the airplane by pulling the control yoke. The CVR also captured statements from both the copilot and pilot expressing surprise that the airplane was not rotating as they expected. CVR and FDR data indicated that between the time of the rotate callout and the airplane reaching the end of the airport terrain, the airspeed increased to about 120 knots, the weight-on-wheels (WOW) remained in an on-ground state, and the elevator position increased to a maximum value of about +16° ANU. However, the airplane’s pitch attitude minimally changed. After the airplane cleared the end of the airport terrain where the ground elevation decreased 20 to 25 ft, FDR data indicate that the WOW transitioned to air mode with near-full ANU elevator control input, and the airplane pitched up nearly 22° in less than 2 seconds. FDR data depicted forward elevator control input in response to the rapid pitch-up, and the CVR recorded a stall warning then stick shaker activation. An off airport witness reported seeing the front portion of the right engine impact a nearby pole past the departure end of the runway. The airplane then rolled right to an inverted attitude, impacted the ground, then impacted an off airport occupied building. The airplane was destroyed by impact forces and a post crash fire and all four occupants were killed. On ground, four other people were injured, one seriously.
Probable cause:
The pilot-in-command’s failure to release the parking brake before attempting to initiate the takeoff, which produced an unexpected retarding force and airplane-nose-down pitching moment that prevented the airplane from becoming airborne within the takeoff distance available and not before the end of the airport terrain. Contributing to the accident were the airplane’s lack of a warning that the parking brake was not fully released and the Federal Aviation Administration’s process for certification of a derivative aircraft that did not identify the need for such an indication.