Crash of a Gulfstream GIV in Fort Lauderdale
Date & Time:
Aug 21, 2021 at 1340 LT
Registration:
N277GM
Survivors:
Yes
Schedule:
Fort Lauderdale – Las Vegas
MSN:
1124
YOM:
1989
Crew on board:
4
Crew fatalities:
Pax on board:
10
Pax fatalities:
Other fatalities:
Total fatalities:
0
Captain / Total hours on type:
3120.00
Copilot / Total hours on type:
204
Aircraft flight hours:
12990
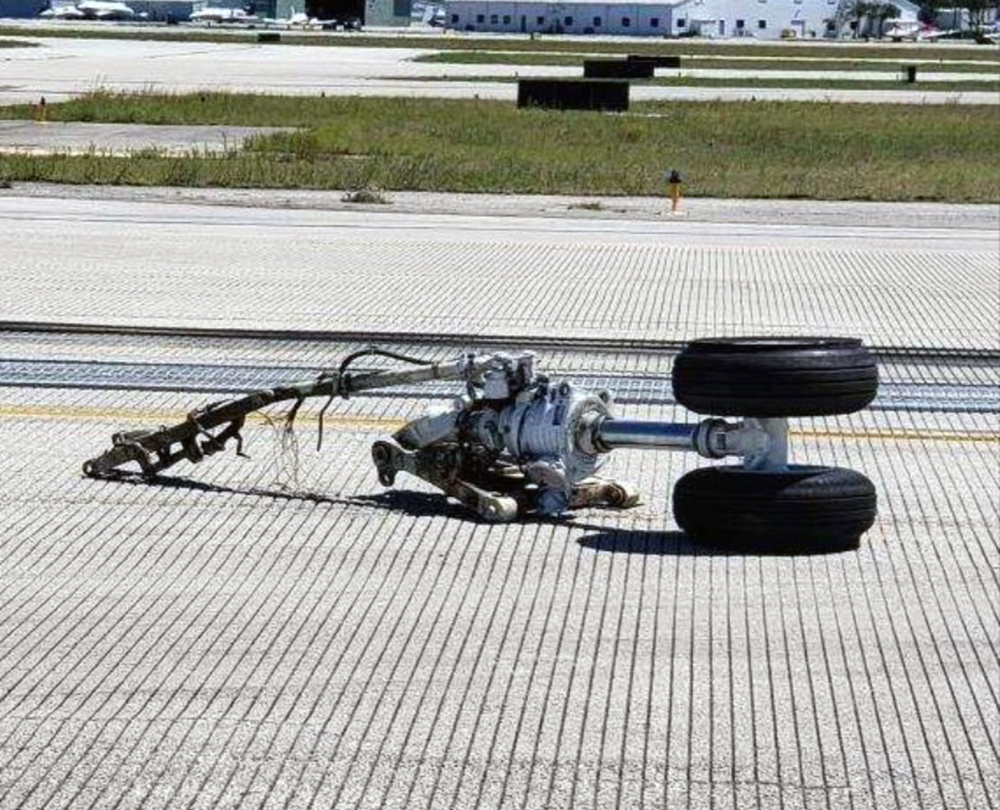
Circumstances:
The flight crew, which consisted of the pilot- and second-in-command (PIC and SIC), and a non-type-rated observer pilot, reported that during takeoff near 100 knots a violent shimmy developed at the nose landing gear (NLG). The PIC aborted the takeoff and during the abort procedure, the NLG separated. The airplane veered off the runway, and the right wing and right main landing gear struck approach lights, which resulted in substantial damage to the fuselage and right wing. The passengers and flight crew evacuated the airplane without incident through the main cabin door. Postaccident interviews revealed that following towing operations prior to the flight crew’s arrival, ground personnel were unable to get the plunger button and locking balls of the NLG’s removable pip pin to release normally. Following a brief troubleshooting effort by the ground crew, the pip pin’s plunger button remained stuck fully inward, and the locking balls remained retracted. The ground crew re-installed the pip pin through the steering collar with the upper torque link arm connected. However, with the locking balls in the retracted position, the pin was not secured in position as it should have been. Further, the ground personnel could not install the safety pin through the pip pin because the pin’s design prevented the safety pin from being inserted if the locking balls and plunger were not released. The ground personnel left the safety pin hanging from its lanyard on the right side of the NLG. The ground personnel subsequently informed their ramp supervisor of the anomaly. The supervisor reported that he informed the first arriving crewmember at the airplane (the observer pilot) that the nose pin needed to be checked. However, all three pilots reported that no ground crewmember told them about any issues with the NLG or pins. Examination of the runway environment revealed that the first item of debris located on the runway was the pip pin. Shortly after this location, tire swivel marks were located near the runway centerline, which were followed by large scrape and tire marks, leading to the separated NLG. The safety pin remained attached to the NLG via its lanyard and was undamaged. Postaccident examination and testing of the NLG and its pins revealed no evidence of preimpact mechanical malfunctions or failures. The sticking of the pip pin plunger button that the ground crew reported experiencing could not be duplicated during postaccident testing. When installed on the NLG, the locking ball mechanism worked as intended, and the pip pin could not be removed by hand. Although the airplane’s preflight checklist called for a visual check of the NLG’s torque link to ensure that it was connected to the steering collar by the pip pin and that the safety pin was installed, it is likely that none of the pilots noticed that the pip pin did not have its safety pin installed during preflight. Subsequently, during the takeoff roll, without the locking balls extended, the pip pin likely moved outward and fell from its position holding the upper torque link arm. This allowed the upper torque link arm to move freely, which resulted in the violent shimmy and NLG separation. The location of the debris on the runway, tire marks, and postaccident examination and testing support this likely chain of events. Contributing to the PIC and SIC’s omission during preflight was the ground crew’s failure to directly inform the PIC or SIC that there was a problem with the NLG pip pin. The ground crew also failed to discard the malfunctioning pip pin per the airplane’s ground handling procedures and instead re-installed the pip pin. Although the observer pilot was reportedly informed of an issue with a nose gear pin, he was not qualified to act as a required flight crewmember for the airplane and was on his cell phone when he was reportedly informed of the issue by the ramp supervisor. These factors likely contributed to the miscommunication and the PIC’s and SIC’s subsequent lack of awareness of the NLG issue.
Probable cause:
The pilot-in-command’s (PIC) and second-in-command’s (SIC) failure during preflight inspection to ensure that the nose landing gear’s pip pin was properly installed, which resulted in separation of the pip pin during takeoff. Contributing to the accident was the ground crew supervisor’s failure to inform the PIC or SIC of the anomaly concerning the pip pin following a towing operation.
Final Report: