Crash of a Cessna 208B Grand Caravan in Oceanside: 1 killed
Date & Time:
Jun 3, 2022 at 1347 LT
Operator:

Registration:
N7581F
Survivors:
Yes
Schedule:
Oceanside - Oceanside
MSN:
208B-0389
YOM:
1994
Crew on board:
2
Crew fatalities:
Pax on board:
0
Pax fatalities:
Other fatalities:
Total fatalities:
1
Captain / Total hours on type:
161.00
Copilot / Total hours on type:
25
Aircraft flight hours:
13379
Circumstances:
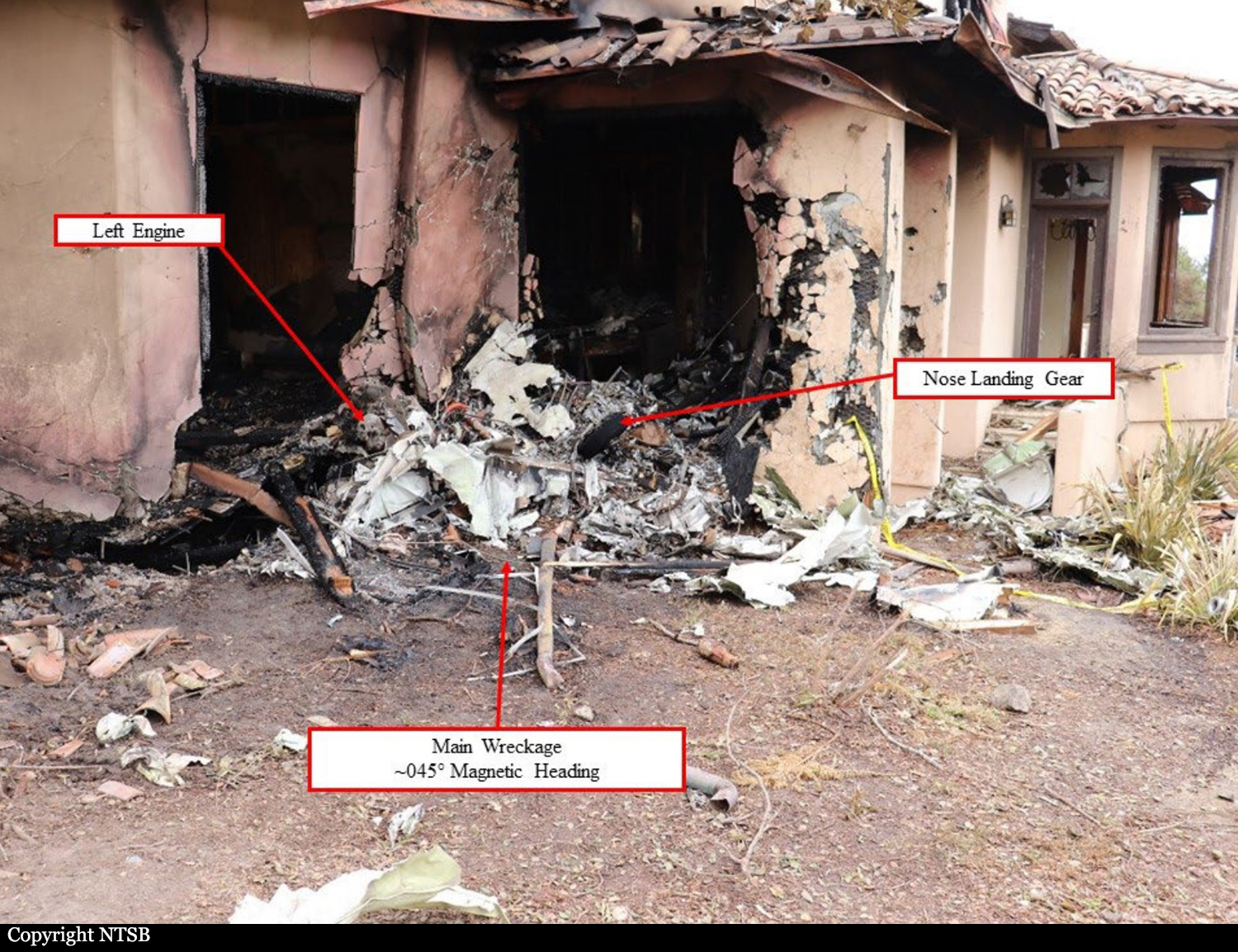
The pilots were performing skydiving flights while the right-seated pilot was training the left-seated pilot on the operation. The pilots completed six flights without incident and completed the drop of the skydivers on the accident flight normally. The right-seated pilot could not completely recollect the minutes leading up to the accident due to his injuries. He did recall that airplane was descending as expected with the power at idle. The recorded ADS-B data revealed that after turning onto final approach, the airplane then completed a right 360° turn presumably because the altitude was too high. The right-seated pilot attempted to increase the power by slightly nudging the throttle forward and thought the engine power did not increase as expected. A performance study revealed that in the last 70 seconds of recorded data, the airplane underwent a series of speed and thrust oscillations consistent with a pilot increasing and then decreasing the power lever. The right seat pilot recalls aiming for an open dirt field and observing a berm in the immediate flight path. In an effort to avoid the berm, he maneuvered the airplane into a right turn. The airplane landed short of the runway, resulting in a collision with the berm. The engine was producing power at the time of impact. Postaccident examination of the airplane revealed no evidence of mechanical malfunctions or failures that would have precluded normal operation. The right-seated pilot was in the process of training the left-seated pilot and stated that he took over the controls during the final approach. It is unknown when he took over the controls, so it is unknown which pilot was at the controls during the speed oscillations. The right-seated pilot likely took over the controls too late and the airplane impacted the terrain. The left-seated pilot’s ability to hear the changes in engine power might have been hindered because she was listening to music through her headset at an elevated decibel level. The airplane was modified by a Supplemental Type Certificate that replaces the original Pratt & Whitney PT-6 turbine engine with a Honeywell TPE331 turbine engine. The TPE331 engine’s characteristics are such that if the airplane is on final approach with the power near idle, the throttle sensitivity (change in thrust per unit of power lever movement) increases around the transition between the propellergoverning and underspeed-governing modes of the engine, which corresponds to a zero-thrust condition. Near this transition point, small movements of the power lever (about ¼ to ½ inch of deflection) can result in relatively large thrust changes that can surprise pilots inexperienced with this behavior and result in pilot-induced oscillations (PIO). Given the thrust oscillations observed shortly before the end of the ADS-B data, it is likely that the left-seated pilot was at the controls and experienced such a PIO on a short final approach to land.
Probable cause:
The right-seated pilot’s failure to correct the left-seated pilot’s mismanagement of the engine thrust, which resulted in undesired speed and thrust oscillations during the final approach and a subsequent descent into terrain.
Final Report: