Country
Crash of a Fokker 50 in Sharjah: 43 killed
Date & Time:
Feb 10, 2004 at 1138 LT
Operator:

Registration:
EP-LCA
Survivors:
Yes
Schedule:
Kish Island - Sharjah
MSN:
20273
YOM:
1993
Flight number:
IRK1770
Crew on board:
6
Crew fatalities:
Pax on board:
40
Pax fatalities:
Other fatalities:
Total fatalities:
43
Captain / Total hours on type:
1516.00
Copilot / Total hours on type:
517
Aircraft flight hours:
20466
Aircraft flight cycles:
19845
Circumstances:
The aircraft was operating as a scheduled flight from Kish Island, Iran to Sharjah, UAE with the captain initially as the pilot flying (PF). During the cruise and just prior to descent, the captain unexpectedly handed over control of the aircraft to the First Officer prior to the approach to Sharjah. The first officer did not accept this willingly and stated that he was not confident of his ability to conduct a VOR/DME approach into Sharjah. This statement was not consistent with his previous experience and could indicate either a cultural or professional issue. The captain insisted the first officer fly the aircraft and encouraged and instructed him during the approach. At 11:24 hours local time, the aircraft contacted Dubai Arrivals and was cleared from 9000 ft to 5000 ft and instructed to expect a VOR/DME approach to runway 12 at Sharjah International Airport. At 11:29 hours the aircraft was further cleared to 2500 ft and cleared for the approach. The aircraft was under its own navigation and the daylight conditions were fine with excellent visibility. At 11:35 hours the aircraft was instructed to contact Sharjah Tower and the pilot reported that the aircraft was established on the VOR final approach for runway 12. The Tower cleared IRK7170 to land and advised that the wind was calm. At that point the aircraft was slightly above the approach profile. The initial speed for the approach was at least 50 kt high at approximately 190 kt with no flap and no landing gear. The aircraft should have been configured with landing gear down and flap 10° during the approach and stabilized at 130 kt prior to the MDA. Approaching the MDA at flight idle setting, the autopilot was disengaged and the first Officer called for flap 10 at 186 kt (limiting speed of 180 kt) and flap 25 was selected by the Captain, a setting uncalled for by the Pilot Flying at 183 kt (limiting speed of 160 kt), and the landing gear was called for and selected at approximately 185 kt (limiting speed of 170 kt). The captain then took control of the aircraft and shortly afterwards the ground range selectors were heard by Cockpit Voice Recorder to be lifted and the power levers moved from the flight idle stop into the ground control range. The left propeller then went to full reverse whilst the right propeller remained in positive pitch within the ground control range. The aircraft descended in an extreme nose low left bank attitude until impact. The aircraft crashed 2.6 nm from the runway onto an unprepared sandy area adjacent to a road and residential buildings. The aircraft broke apart on impact and a fire started immediately. Three passengers suffered injuries while 43 other occupants were killed.
Probable cause:
During the final approach, the power levers were moved by a pilot from the flight idle position into the ground control range, which led to an irreversible loss of flight control. The following contributing factors were identified:
1. By suddenly insisting the First Officer fly the final approach, the pilot in command created an environment, which led to a breakdown of crew resource management processes, the non observance of the operator’s standard operating procedures and a resultant excessive high approach speed.
2. An attempt to rectify this excessive high approach speed most likely resulted in the non compliance with the Standard Operating Procedures and the movement of the power levers below flight idle.
3. The unmodified version of the Skid Control Unit failed to provide adequate protection at the time of the event.
1. By suddenly insisting the First Officer fly the final approach, the pilot in command created an environment, which led to a breakdown of crew resource management processes, the non observance of the operator’s standard operating procedures and a resultant excessive high approach speed.
2. An attempt to rectify this excessive high approach speed most likely resulted in the non compliance with the Standard Operating Procedures and the movement of the power levers below flight idle.
3. The unmodified version of the Skid Control Unit failed to provide adequate protection at the time of the event.
Final Report:




























Crash of a Fokker 50 in Adar Yeil
Date & Time:
Jun 16, 2003 at 0630 LT
Operator:

Registration:
ST-ARA
Survivors:
Yes
Schedule:
Khartoum - Adar Yeil
MSN:
20154
YOM:
1989
Crew on board:
3
Crew fatalities:
Pax on board:
42
Pax fatalities:
Other fatalities:
Total fatalities:
0
Circumstances:
After landing on a gravel runway at Adar Yeil Airport, the aircraft collided with a flock of birds, damaging the left engine. The aircraft went out of control and veered to the left, causing the left propeller to struck the ground. The propeller blades separated, punctured the fuselage and injured three passengers. The aircraft came to a halt and all occupants evacuated. The aircraft was damaged beyond repair.
Probable cause:
Loss of control after landing following a collision with a flock of birds.
Crash of a Fokker 50 in Mellila
Date & Time:
Jan 17, 2003 at 1201 LT
Operator:

Registration:
PH-FZE
Survivors:
Yes
Schedule:
Málaga – Melilla
MSN:
20182
YOM:
1990
Flight number:
YW8276
Crew on board:
5
Crew fatalities:
Pax on board:
14
Pax fatalities:
Other fatalities:
Total fatalities:
0
Captain / Total hours on type:
3500.00
Copilot / Total hours on type:
64
Aircraft flight hours:
22534
Aircraft flight cycles:
25803
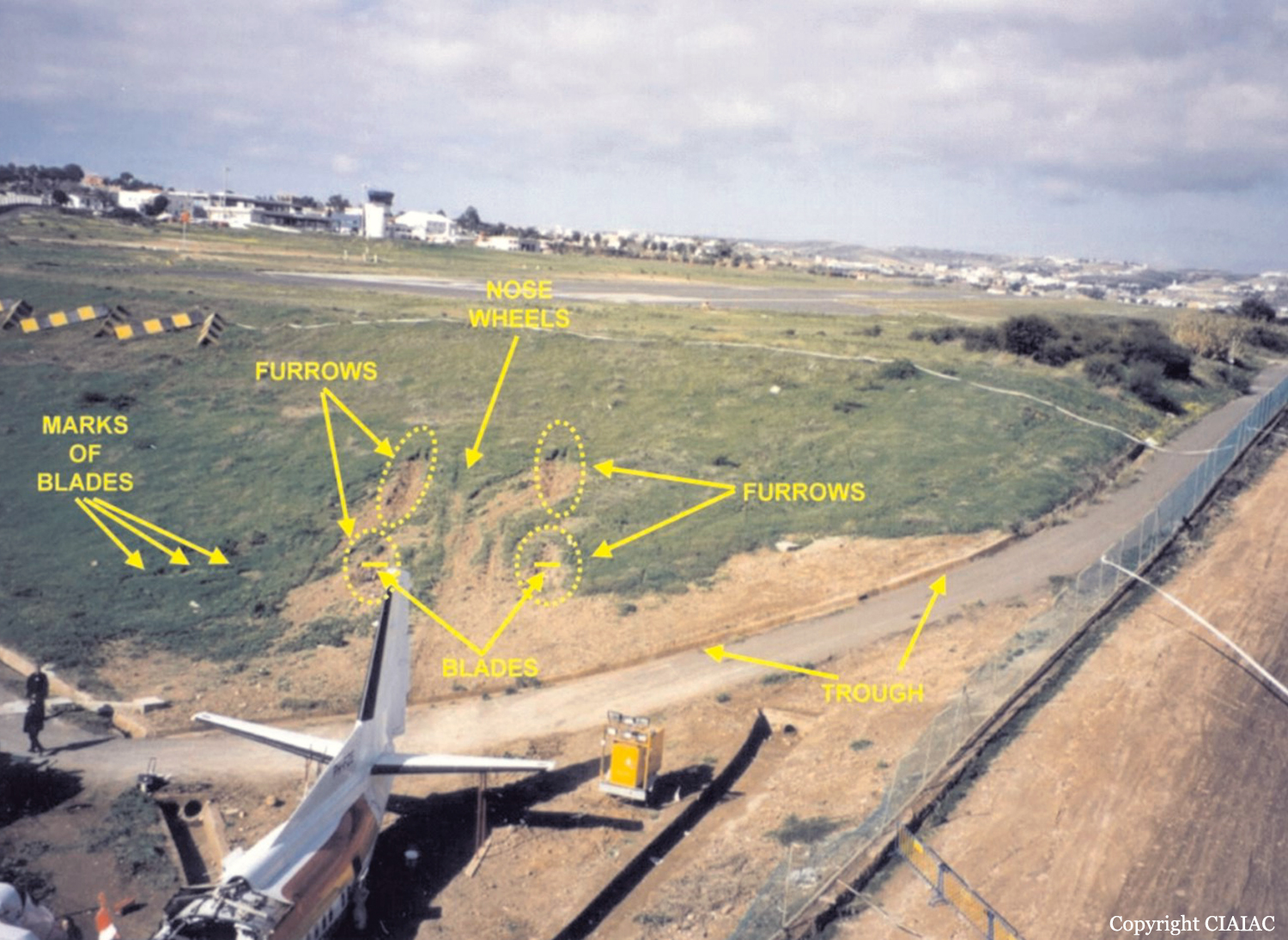
Circumstances:
After landing on runway 15 at Melilla Airport, the pilot-in-command noticed that he could not engage the ground idle/reverse of both propellers, and that the aircraft did not brake normally. The aircraft started to deviate to the left of the runway axis while both pilots were applying brakes. After tyre n°3 burst, the deviation continued until the aircraft left the paved surface of the runway and finally fell through an embankment with around 15 metres of height located at the end of runway 15. The aircraft was destroyed and the pilot-in-command and other nine people suffered minor injuries. There was no fire.
Probable cause:
It is considered that the accident probably happened because of a combination of three factors:
1. An unstable approach that resulted in a higher than normal touchdown speed.
2. The inability to select propeller reverse due to the probable tripping of the circuit breaker FLIGHT IDLE SOLENOID 1 & 2 before or at touchdown.
3. The cross connection of the wheel speed transducer wire harness of wheels 3 and 4, which, due to heavy braking, produced a flat spot in wheel 3 and reduced the braking capability of wheel 4.
1. An unstable approach that resulted in a higher than normal touchdown speed.
2. The inability to select propeller reverse due to the probable tripping of the circuit breaker FLIGHT IDLE SOLENOID 1 & 2 before or at touchdown.
3. The cross connection of the wheel speed transducer wire harness of wheels 3 and 4, which, due to heavy braking, produced a flat spot in wheel 3 and reduced the braking capability of wheel 4.
Final Report:





Crash of a Fokker 50 in Luxembourg: 20 killed
Date & Time:
Nov 6, 2002 at 1006 LT
Operator:

Registration:
LX-LGB
Survivors:
Yes
Schedule:
Berlin – Luxembourg
MSN:
20221
YOM:
1991
Flight number:
LG9642
Crew on board:
3
Crew fatalities:
Pax on board:
19
Pax fatalities:
Other fatalities:
Total fatalities:
20
Captain / Total hours on type:
2864.00
Copilot / Total hours on type:
443
Aircraft flight hours:
21836
Aircraft flight cycles:
24068
Circumstances:
The Fokker 27 Mk050 registered LX-LGB and operated by Luxair left Berlin on 6 November 2002 at 07h 40min on flight LG 9642/LH 2420 with destination Luxembourg. Cruising level was at FL180. At 08h 50min, Frankfurt Control asked the crew to stop descent at FL 90, direct to Diekirch and at 08h 52min the flight was transferred to Luxembourg Approach. They were instructed to enter the Diekirch hold at FL90, to expect later on vectors for an ILS 24 and were given the latest RVR readings. At 08h 59min, well before reaching the Diekirch hold, the aircraft was recleared to 3000ft QNH and to turn left heading one three zero. At this time the aircraft flew in the clear sky above a fog layer. RVR was two hundred seventy five meters. The crew evoked a go-around if the RVR was not three hundred meters whilst passing ELU (it’s minima for a category II approach). At 09h04 min 36s, the aircraft passed overhead ELU maintaining 3000ft QNH. At 09h04 min 57s, the ATC controller transmitted an RVR of three hundred meters. Power was further reduced, flaps 10 were selected and the landing gear was lowered. Immediately after the landing gear was lowered, the pitch angle of the two propellers simultaneously reached a value that is lower than the minimum values for flight. This propeller pitch setting involves a rapid decrease of speed and altitude. During the following seconds, the left engine stopped and then the right engine stopped. The flight data recorders, no longer powered ceased functioning. At 09h05 min 42s (radar time base), the aircraft disappeared from the radar screen. It was immediately found in a field seven hundred meters to the north of runway centreline 24 and three point five kilometres to the east of the threshold. Six people were critically injured while 16 others were killed. Within the following hours, four of the survivors died from their injuries. The only two survivors were a passenger, a French citizen, and the captain.
Probable cause:
The initial cause of the accident is the crew’s acceptance of the approach clearance although they were not prepared to it, namely the absence of preparation of a go-around. It led the crew to perform a series of improvised actions that ended in the prohibited override of the primary stop on the power levers and leading to an irreversible loss of control.
Contributory factors can be listed as follows:
1. A lack of preparation for the landing, initiated by unnecessary occupations resulting from an obtained RVR value, which was below their company approved minima, created a disorganisation in the cockpit, leading to uncoordinated actions by each crewmember.
2. Some procedures as laid down in the operations manual were not followed at some stage of the approach. All this did not directly cause the accident, but created an environment whereby individual actions were initiated to make a landing possible.
3. Routine and the will to arrive at destination may have put the crew in a psychological state of mind, which could have been the origin of the deviations from standard procedures as noticed.
4. The priority in the approach sequence given to the crew by ATC, which facilitated the traffic handling for the controller who was not aware of the operational consequences.
5. The low reliability of the installed secondary stop safety device that was favoured by the non-application of service bulletin ABSC SB Fo50-32-4. Also the mode of distribution of the safety information (Fokker Aircraft B.V. – Service letter 137) to the operator as well as the operator’s internal distribution to the crews, that did not guarantee that the crews were aware of the potential loss of secondary stop on propeller pitch control.
6. Latent shortcomings in the Authority and the organisational structure of the operator, in combination with poor application of SOPs by the crew.
Contributory factors can be listed as follows:
1. A lack of preparation for the landing, initiated by unnecessary occupations resulting from an obtained RVR value, which was below their company approved minima, created a disorganisation in the cockpit, leading to uncoordinated actions by each crewmember.
2. Some procedures as laid down in the operations manual were not followed at some stage of the approach. All this did not directly cause the accident, but created an environment whereby individual actions were initiated to make a landing possible.
3. Routine and the will to arrive at destination may have put the crew in a psychological state of mind, which could have been the origin of the deviations from standard procedures as noticed.
4. The priority in the approach sequence given to the crew by ATC, which facilitated the traffic handling for the controller who was not aware of the operational consequences.
5. The low reliability of the installed secondary stop safety device that was favoured by the non-application of service bulletin ABSC SB Fo50-32-4. Also the mode of distribution of the safety information (Fokker Aircraft B.V. – Service letter 137) to the operator as well as the operator’s internal distribution to the crews, that did not guarantee that the crews were aware of the potential loss of secondary stop on propeller pitch control.
6. Latent shortcomings in the Authority and the organisational structure of the operator, in combination with poor application of SOPs by the crew.
Final Report:






















