Country
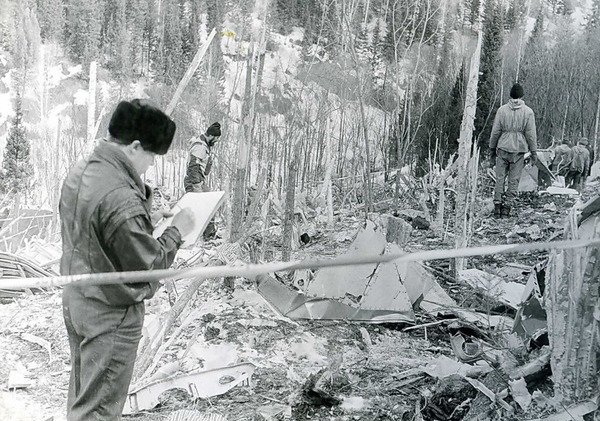
Crash of an Airbus A310-308 near Mezhdurechensk: 75 killed
Date & Time:
Mar 23, 1994 at 0057 LT
Operator:

Registration:
F-OGQS
Survivors:
No
Schedule:
Moscow - Hong Kong
MSN:
596
YOM:
1991
Flight number:
SU593
Crew on board:
12
Crew fatalities:
Pax on board:
63
Pax fatalities:
Other fatalities:
Total fatalities:
75
Captain / Total hours on type:
38.00
Copilot / Total hours on type:
440
Aircraft flight hours:
5375
Aircraft flight cycles:
846
Circumstances:
While cruising by night at the assigned altitude of 10,100 metres, approaching the Novokuznetsk reporting point, the captain's daughter entered the cockpit. She was allowed to sit the left-hand seat while the captain demonstrated some autopilot features, using HDG/S and NAV submodes to alter the heading. The captain's son then took the left front seat. The captain intended to demonstrate the same manoeuvre when his son asked if he could turn the control wheel. He then turned the wheel slightly (applying a force of between 8-10 kg) and held it in that position for a few seconds before returning the wheel to the neutral position. The captain then demonstrated the same features as he did to his daughter and ended by using the NAV submode to bring the aircraft back on course. As the autopilot attempted to level the aircraft at its programmed heading, it came in conflict with the inputs from the control wheel which was blocked in a neutral position. Forces on the control wheel increased to 12-13 kg until the torque limiter activated by disconnecting the autopilot servo from the aileron control linkage. The autopilot remained engaged however. The aircraft then started to bank to the right at 2,5° per second, reaching 45° when the autopilot wasn't able to maintain altitude. The A310 started buffeting, which caught the attention of the captain who told the copilot to take control while he was trying to regain his seat. The seat of the copilot was fully aft, so it took him an additional 2-3 seconds to get to the control wheel. The bank continued to 90°, the aircraft pitched up steeply with +4,8g accelerations, stalled and entered a spin. Two minutes and six seconds later the aircraft struck the ground. The aircraft disintegrated on impact and all 75 occupants were killed, among them 25 foreigners.
Probable cause:
The accident was caused by a stall, spin and impact with the ground resulting from a combination of the following factors:
1. The decision by the PIC to allow an unqualified and unauthorized outsider (his son) to occupy his duty station and intervene in the flying of the aeroplane.
2. The execution of demonstration manoeuvres that were not anticipated in the flight plan or flight situation, with the PIC operating the autopilot while not at his duty station.
3. Application by the outsider and the co-pilot of control forces that interfered with the functioning of the roll channel of the autopilot (and are not recommended in the A310 flight manual), thus overriding the autopilot and disconnecting it from the aileron control linkage.
4. The copilot and PIC failed to detect the fact that the autopilot had become disconnected from the aileron control linkage, probably because:
- The A310 instrumentation has no declutch warning. The provision of signals in accordance with the requirements of Airworthiness Standard NLGS-3, para. 8.2.7.3., and international recommended practices, could have enabled the crew to detect the disengaged autopilot in a timely manner.
- The copilot and PIC may have been unaware of the peculiarities of the declutching function and the actions to be taken in such a situation because of a lack of appropriate information in the flight manual and crew training programme;
- It was difficult for the co-pilot to detect the disengagement of the autopilot by feel, either because of the small forces on his control column or because he took changing forces to be the result of Eldar's actions;
- The PIC was away from his position and distracted by the conversation with his daughter.
5. A slight, unintentional further turn of the control wheel(s) following disengagement of the autopilot caused a right roll to develop.
6. The PIC and copilot failed to detect the excessive right bank angle, which exceeded operating limits, and were late in re-entering the aircraft control loop because their attention was focussed on determining why the aircraft had banked to the right, a manoeuvre they interpreted as entry into a holding area with either no course line or with a new (false) course line generated on the navigational display.
A strong signal indicating that the aeroplane had exceeded the allowable operating bank angle, taking account of the delay in recognizing and assessing the situation and making a decision, could in this situation have attracted the crew's attention and enabled them to detect the bank at an earlier stage.
7. The aeroplane was subjected to buffeting and high angles of attack because the autopilot continued to perform its height-keeping function even after the actuator declutched and as the right roll developed, until the pilot disconnected it by overriding its longitudinal channel.
8. Inappropriate and ineffective action on the part of the copilot, who failed to disconnect the autopilot and to push the control column forward when the buffeting occurred and the aeroplane entered an unusual attitude (high angles of attack and pitch). These actions, which caused the aeroplane to stall and spin, could have resulted from:
- the presence of an outsider in the left-hand pilot's seat and the resulting delay before the PIC re-entered the aeroplane control loop;
- the less-than-optimum working posture of the copilot, whose seat was pushed back to its rearmost position;
- the occurrence, 2 seconds following the onset of buffeting, of an unintentional pitching up of the aeroplane, which sharply increased the angle of attack and reduced lateral controllability;
- unpreparedness of the crew to act in this situation because of lack of appropriate drills in the training programme;
- temporary loss of spatial orientation in night conditions.
1. The decision by the PIC to allow an unqualified and unauthorized outsider (his son) to occupy his duty station and intervene in the flying of the aeroplane.
2. The execution of demonstration manoeuvres that were not anticipated in the flight plan or flight situation, with the PIC operating the autopilot while not at his duty station.
3. Application by the outsider and the co-pilot of control forces that interfered with the functioning of the roll channel of the autopilot (and are not recommended in the A310 flight manual), thus overriding the autopilot and disconnecting it from the aileron control linkage.
4. The copilot and PIC failed to detect the fact that the autopilot had become disconnected from the aileron control linkage, probably because:
- The A310 instrumentation has no declutch warning. The provision of signals in accordance with the requirements of Airworthiness Standard NLGS-3, para. 8.2.7.3., and international recommended practices, could have enabled the crew to detect the disengaged autopilot in a timely manner.
- The copilot and PIC may have been unaware of the peculiarities of the declutching function and the actions to be taken in such a situation because of a lack of appropriate information in the flight manual and crew training programme;
- It was difficult for the co-pilot to detect the disengagement of the autopilot by feel, either because of the small forces on his control column or because he took changing forces to be the result of Eldar's actions;
- The PIC was away from his position and distracted by the conversation with his daughter.
5. A slight, unintentional further turn of the control wheel(s) following disengagement of the autopilot caused a right roll to develop.
6. The PIC and copilot failed to detect the excessive right bank angle, which exceeded operating limits, and were late in re-entering the aircraft control loop because their attention was focussed on determining why the aircraft had banked to the right, a manoeuvre they interpreted as entry into a holding area with either no course line or with a new (false) course line generated on the navigational display.
A strong signal indicating that the aeroplane had exceeded the allowable operating bank angle, taking account of the delay in recognizing and assessing the situation and making a decision, could in this situation have attracted the crew's attention and enabled them to detect the bank at an earlier stage.
7. The aeroplane was subjected to buffeting and high angles of attack because the autopilot continued to perform its height-keeping function even after the actuator declutched and as the right roll developed, until the pilot disconnected it by overriding its longitudinal channel.
8. Inappropriate and ineffective action on the part of the copilot, who failed to disconnect the autopilot and to push the control column forward when the buffeting occurred and the aeroplane entered an unusual attitude (high angles of attack and pitch). These actions, which caused the aeroplane to stall and spin, could have resulted from:
- the presence of an outsider in the left-hand pilot's seat and the resulting delay before the PIC re-entered the aeroplane control loop;
- the less-than-optimum working posture of the copilot, whose seat was pushed back to its rearmost position;
- the occurrence, 2 seconds following the onset of buffeting, of an unintentional pitching up of the aeroplane, which sharply increased the angle of attack and reduced lateral controllability;
- unpreparedness of the crew to act in this situation because of lack of appropriate drills in the training programme;
- temporary loss of spatial orientation in night conditions.
Final Report:












Crash of an Airbus A310-304 near Kathmandu: 113 killed
Date & Time:
Jul 31, 1992 at 1245 LT
Operator:

Registration:
HS-TID
Survivors:
No
Schedule:
Bangkok - Kathmandu
MSN:
438
YOM:
1987
Flight number:
TG311
Crew on board:
14
Crew fatalities:
Pax on board:
99
Pax fatalities:
Other fatalities:
Total fatalities:
113
Circumstances:
Thai Airways Flight 311 was conducting the Sierra (VOR/DME) approach to runway 02 at Tribhuvan International Airport, in instrument weather conditions. A flap fault occurred while the flight was on the approach; this caused the crew to ask for clearance back to Calcutta, a decision that was in keeping with both Company and performance requirements, which necessitate the use of full flaps for the steep final approach. Shortly (21 seconds) after making this request, at a distance of approximately 12 nm from the Kathmandu VOR, the flap fault was rectified by retracting and then reselecting the flaps. The crew determined that it was not possible to continue the straight-in approach, due to the steep descent angles required and the position of the aircraft. The crew stated to the control tower that they wished to start their approach again and requested a left turn back to the Romeo fix, which is 41 nm south south-west (202 radial) of the Kathmandu VOR. The Controller, in the non-radar environment, responded by clearing the flight to make the Sierra approach, which starts at the 202 radial and 16 nautical miles from the VOR. The crew response to the clearance was to report that, at the moment, they couldn't land and to ask again for left turn back to Romeo to start their approach again. After further dialogue with the controller, which included requests for a left turn, the crew unilaterally initiated a right turn from the aircraft's 025° heading and commenced a climb from an altitude of 10,500 feet to FL180, when the flight was about 7 nm south of the Kathmandu VOR. The crew reported to the tower controller that the flight was climbing and the controller replied by instructing the crew to report at 16 nm for the Sierra approach. During the turn, there was more discussion between the tower controller and the flight, where it was established that the aircraft was to maintain an altitude of FL115 and was to 'proceed to Romeo' and contact the Area Control Center (ACC) controller. The flight, commencing a descent while in the turn, completed a 360° turn, momentarily rolling out on headings of 045° and 340°, and again proceeded toward the north on a heading of 025° magnetic. When the flight was about 5 nm south-west of the Kathmandu VOR, the crew contacted the ACC and stated that the aircraft was 'heading 025' and they wished to proceed to Romeo to start their approach again; adding they had 'technical problems concerned with the flight.' It was again established that the flight was to proceed to Romeo and the crew agreed to 'report over Romeo.' It was determined from the cockpit voice recorder that the crew was in the process of inserting 'Romeo' and other related navigational information in the Flight Management System, but were experiencing difficulties. The flight continued towards the north on a heading of 025° and then, at about 16 nm north, the heading was altered to the left to 005°. Slightly over one minute later, the Ground Proximity Warning System (GPWS) sounded the warning 'terrain, terrain' followed by 'whoop whoop pull-up'; the aural warning continued until impact approximately 16 seconds later. Engine thrust was increasing and 'Level Change' had been announced on the cockpit, just before the impact occurred at the 11,500-foot level of a 16,000-foot peak; the accident site was located on the 015 radial (north-north east) at 23.3 nm from the Kathmandu VOR. The aircraft was destroyed and all 113 occupants were killed.
Probable cause:
TG311 flight crew's management of the aircraft flight path wherein the flight proceeded in a northerly direction which was opposite to the cleared point Romeo to the South; ineffective radio communication between the area control centre and the TG311 flight crew which allowed the flight to continue in the wrong direction, in that the TG311 crew never provided the aircraft's VOR radial when stating DME and the controller never solicited this information and thus the aircraft's position was not transmitted at any time; and ineffective cockpit crew coordination by the TG311 crew in conducting flight navigation duties. Contributing factors were: the misleading depiction of Romeo on the operator's approach chart used by the flight crew; a flap fault, although corrected, required that the initial approach be discontinued; and radio communication difficulties between the TG311 crew and the air traffic controllers that stemmed from language difficulties and ineffective discussion of apparent unresolved problems.


