

Country
Crash of a Tupolev TU-154M in Wenzhou: 61 killed
Date & Time:
Feb 24, 1999 at 1634 LT
Operator:

Registration:
B-2622
Survivors:
No
Schedule:
Chengdu - Wenzhou
MSN:
90A846
YOM:
1990
Flight number:
SZ4509
Crew on board:
11
Crew fatalities:
Pax on board:
50
Pax fatalities:
Other fatalities:
Total fatalities:
61
Aircraft flight hours:
14135
Aircraft flight cycles:
7748
Circumstances:
Following an uneventful flight from Chengdu, the crew was cleared to descend to Wenzhou Airport. While passing 9,000 metres on descent, the crew encountered technical difficulties with the control column that was too far forward. At 1629LT, the crew was cleared to descend from 1,200 to 700 metres when the aircraft entered a nose-down attitude. Flaps were selected down (first stage) when the AOA alarm sounded in the cockpit. The aircraft entered an uncontrolled descent and crashed in an open field. It disintegrated on impact and all 61 occupants were killed. Several farmers were injured by debris.
Probable cause:
A self-locking nut, other than castle nut with cotter pin as specified, had been installed at the bolt for connection between pull rod and bellcranck in the elevator control system. The nut screwed off, resulting in bolt loss, which led to the loss of pitch control.




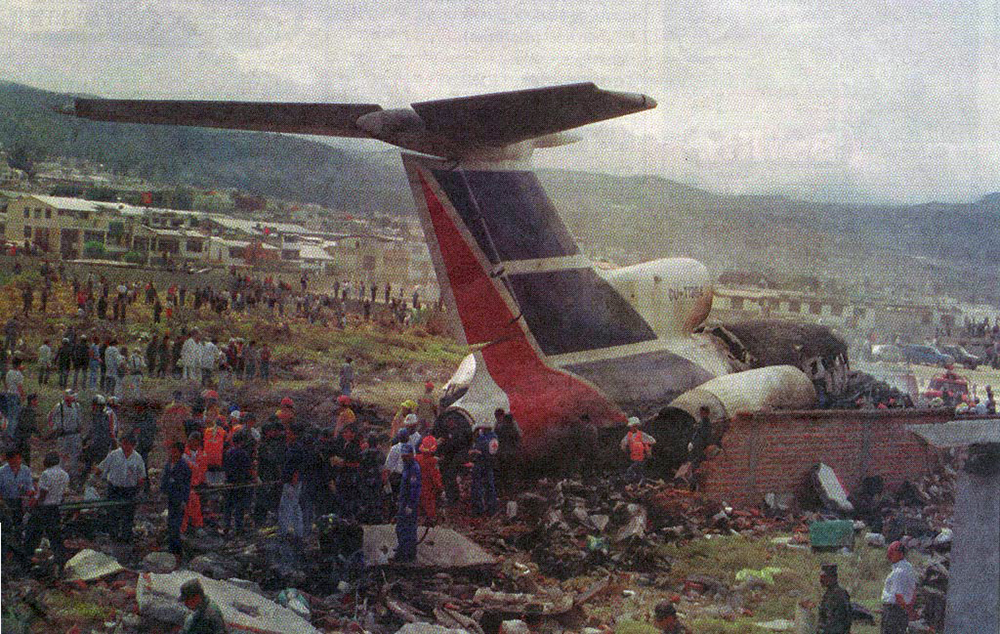
Crash of a Tupolev TU-154M in Quito: 80 killed
Date & Time:
Aug 29, 1998 at 1303 LT
Operator:

Registration:
CU-T1264
Survivors:
Yes
Schedule:
Quito - Guayaquil - Havana
MSN:
85A720
YOM:
1985
Flight number:
CU389
Crew on board:
14
Crew fatalities:
Pax on board:
77
Pax fatalities:
Other fatalities:
Total fatalities:
80
Aircraft flight hours:
9256
Circumstances:
While parked on the apron at Quito-Mariscal Sucre Airport, the crew started the engine when a pneumatic valve blocked. The problem was resolved and two engines were started with ground power unit while the third engine was started during taxi. During the takeoff roll on runway 17, at Vr speed, the pilot-in-command started the rotation but the aircraft failed to respond. For unknown reasons, the crew took 10 seconds to decide to abort the takeoff. The captain initiated an emergency braking procedure but the remaining distance of 800 metres was insufficient. Unable to stop, the aircraft overran, struck a concrete wall, an auto spare parts building and crashed near a soccer field, bursting into flames. Seventy people in the aircraft was well as 10 people on the ground were killed while 21 people in the airplane and 15 on the ground were injured, some seriously. At the time of the accident, the total weight of the aircraft was 73,309 kilos, within limits.
Probable cause:
It is believed that the crew failed to follow the taxi and pre-takeoff checklist and forgot to select the switches for the hydraulic valves of the control system. No technical anomalies were found on the aircraft and engines.









Crash of a Tupolev TU-154B-1 in Sharjah: 85 killed
Date & Time:
Dec 15, 1997 at 1835 LT
Operator:

Registration:
EY-85281
Survivors:
Yes
Schedule:
Dushanbe - Sharjah
MSN:
78A281
YOM:
1978
Flight number:
TZK3183
Crew on board:
7
Crew fatalities:
Pax on board:
79
Pax fatalities:
Other fatalities:
Total fatalities:
85
Circumstances:
Following an uneventful flight, the aircraft entered the UAE airspace and was cleared by Dubai ATC to successively descend to FL170, 100, 060 and 025 via heading 190. Passing 3,460 feet on descent, the crew was cleared to continue to 1,500 feet when, at an altitude of 1,800 feet, the aircraft entered an area of turbulences. The level of 1,500 feet was reached 15 km from the runway 30 threshold. For unknown reasons, the crew failed to report he was passing 1,500 feet and was then instructed to continue via heading 270 for the final approach to runway 30. In a relative limited visibility, the crew initiated a right turn at a speed of 400 km/h then lowered the landing gear. At an altitude of 820 feet, an alarm sounded in the cockpit, informing the crew about an excessive angle of attack. The captain corrected the pitch from 20° to 14° when few seconds later, at an altitude of 690 feet, the aircraft entered a second area of turbulences. The captain realized his altitude was insufficient and requested an increase of engine power when the aircraft struck the ground and crashed 13 km short of runway, bursting into flames. The copilot was the only survivor while 85 other occupants were killed. The aircraft disintegrated on impact.
Probable cause:
The accident was the consequence of a controlled flight into terrain.
The following findings were identified:
- The crew failed to follow the approach published procedures,
- The crew continued the approach below the MDA until the aircraft collided with terrain,
- The crew failed to proceed to the usual approach briefing and checks,
- Lack of visibility due to the night,
- Crew fatigue,
- Lack of crew mutual crosscheck during descent,
- Lack of crew coordination,
- Turbulences in the approach path,
- Non compliance to published procedures.
The following findings were identified:
- The crew failed to follow the approach published procedures,
- The crew continued the approach below the MDA until the aircraft collided with terrain,
- The crew failed to proceed to the usual approach briefing and checks,
- Lack of visibility due to the night,
- Crew fatigue,
- Lack of crew mutual crosscheck during descent,
- Lack of crew coordination,
- Turbulences in the approach path,
- Non compliance to published procedures.







Crash of a Tupolev TU-154M in the Atlantic Ocean: 24 killed
Date & Time:
Sep 13, 1997 at 1710 LT
Operator:

Registration:
11+02
Survivors:
No
Schedule:
Bonn – Niamey – Windhoek – Cape Town
MSN:
89A813
YOM:
1989
Flight number:
GAF074
Crew on board:
10
Crew fatalities:
Pax on board:
14
Pax fatalities:
Other fatalities:
Total fatalities:
24
Circumstances:
Some 65 nautical miles west off the Namibian coast, a US Air Force Lockheed C-141B Starlifter collided with a German Air Force Tupolev 154M in mid-air. Both aircraft crashed, killing all 33 occupants. The Tupolev 154M (11+02), call sign GAF074, operated on a flight from Cologne/Bonn Airport in Germany to Kaapstad, South Africa. En route refueling stops were planned at Niamey, Niger and Windhoek, Namibia. On board were ten crew members and 14 passengers. The C-141B, (65-9405), call sign REACH 4201, had delivered UN humanitarian supplies to Windhoek and was returning to the U.S. via Georgetown on Ascension Island in the South Atlantic Ocean. On board were nine crew members. GAF074 departed Niamey, Niger at 10:35 UTC. REACH 4201 took off from Windhoek at 14:11 UTC and climbed to its filed for and assigned cruise level of 35,000 feet (FL350). At the same time, GAF074 was not at its filed for cruise level of FL390 but was still at its initially assigned cruise level FL350. Windhoek ATC was in sole and continuous radio contact with REACH 4201, with no knowledge of GAF 074's movement. Luanda ATC was in radio contact with GAF074, but they were not in radio contact with REACH 4201. Luanda ATC did receive flight plans for both aircraft but a departure message for only REACH 4201. At 15:10 UTC both aircraft collided at FL350 and crashed into the sea.
Probable cause:
The primary cause of this accident, in my opinion, was GAF 074 flying a cruise level (FL350) which was not the level they had filed for (FL390). Neither FL350 nor FL390 were the correct cruise levels for that aircraft's magnetic heading according to International Civil Aviation Organization regulations. The appropriate cruise level would have been FL290, FL330, FL370, FL410, etc. A substantially contributing factor was ATC agency Luanda's poor management of air traffic through its airspace. While ATC communications could be improved, ATC agency Luanda did have all the pertinent information it needed to provide critical advisories to both aircraft. If ATC agency Luanda was unable to contact GAF 074, it should have used other communication means (HF radio, telefax or telephone) to contact REACH 4201 through ATC agency Windhoek, as outlined in governing documents. Another substantially contributing factor was the complicated and sporadic operation of the Aeronautical Fixed Telecommunications Network (AFTN). Routing of messages to affected air traffic control agencies is not direct and is convoluted, creating unnecessary delays and unfortunate misroutings. Specifically, ATC agency Windhoek did not receive a flight plan or a departure message on GAF 074, which could have been used by the controllers to identify the conflict so they could have advised REACH 4201. In my opinion, the absence of TCAS was not a cause or substantially contributing factor, but the presence of a fully operational TCAS could have prevented the accident." (William H.C. Schell, jr., Colonel, USAF President, Accident Investigation Board).

Crash of a Tupolev TU-154M in Longyearbyen: 141 killed
Date & Time:
Aug 29, 1996 at 1022 LT
Operator:

Registration:
RA-85621
Survivors:
No
Schedule:
Moscow - Longyearbyen
MSN:
86A742
YOM:
1986
Flight number:
VKO2801
Crew on board:
11
Crew fatalities:
Pax on board:
130
Pax fatalities:
Other fatalities:
Total fatalities:
141
Captain / Total hours on type:
1940.00
Copilot / Total hours on type:
10177
Circumstances:
Vnukovo Airlines flight VKO2801 departed Moscow-Vnukovo Airport at 04:44 UTC bound for Longyearbyen Airport on the Norwegian archipelago of Svalbard. It was a chartered flight with workers and their families to coal mining towns on Svalbard. The flight was uneventful until the start of the descent. Before radio contact with Longyear Information, the crew went through the detailed landing procedure for runway 10. At 09:56, the crew were cleared to start the descent. A little later, the crew received additional information consisting of runway in use 28, wind 230 degrees at 16 knots, visibility more than 10 km, rain showers, clouds: few at 1500 feet, scattered at 2000 feet and broken at 4000 feet, temperature +5°C, dewpoint -0°C and QNH 1005 hPa. (Later changed to 1006 hPa). The crew tried to request runway 10 for landing twice, but the request was not understood as such by Longyear Information due to language difficulties. When the flight was overhead the ADV beacon, at 10:15 hrs, the crew reported their position to Longyear Information and entered the base turn with a bank angle of 22 degrees. At 10:16 hrs, the aircraft came out of this turn on magnetic heading 160 degrees. During the right turn to the base turn, a malfunction occurred in the electric trimming mechanism, which was corrected by the crew. At 10:17, the crew started the turn to bring the aircraft out on the magnetic inbound course 300 degrees, as prescribed by the approach chart. The distance from the airport at this moment was 14 NM (25.9 km), as prescribed by the approach chart, but the lateral deviation from the outbound magnetic course 155 degrees from ADV was 2 NM (3.7 km) to the left. At 10:18, after the radio altimeter aural warning had been activated twice, the co-pilot took the controls and, after 6 seconds, turned the autopilot pitch channel off by 'overriding' it. From then on until the impact, the flight continued in autopilot mode in the roll channel, and in manual mode in the pitch channel. The aircraft passed through the localizer centerline and when the turn had been completed, the aircraft rolled out on a magnetic heading of 290 degrees. At this time, there was a discussion within the crew as to whether or not the final turn had been made at the correct time. The discussion led to the roll out of the turn to final approach and a corrective turn to the right to magnetic heading 306 degrees. At this point, the aircraft was 14.7 NM (27.4 km) from the airport, 2.8 km to the right of the approach centerline, maintaining an altitude of 5000 feet (1520 m ) and the crew increased the flap setting to 28 degrees. The airspeed was reduced to approx. 330 km/hr (180 kts). Instead of intercepting the centerline, the crew continued the flight on the right side, more or less paralleling the localizer course with minor heading changes. At 10:20 the flight made a corrective turn, resulting in a track close to 300 degrees. At this point, the lateral deviation from the approach centerline was 3.7 km to the right. During this corrective turn, the aircraft started descending. At 10:21, the crew made yet another corrective turn to the right. At 10:22:05, the aircraft started turning towards the left. The distance to the airport was 8 NM (14.8 km). On this part of the final approach, the aircraft apparently entered an area of strong turbulence created by the proximity to the mountains. The GPWS then activated 9 seconds before impact. The crew reacted to this by applying power and initiating a pitch-up. At 10:22:23, 7.7 NM (14.2 km) from the airport at an altitude of 2975 feet (907 m), the aircraft collided with the top of the mountain Operafjellet 3.7 km to the right of the approach centerline. All 141 occupants were killed, most of them employees of a local carbon mine and their family members.
Probable cause:
The following findings were reported:
1) There is no Russian procedure for offset localizer approaches modifying the required rule to set the landing course on the HSI.
2) The course selected on both HSIs was 283° even though the approach course is 300°. This setting does not affect the indication of the CDI. However, the CDI was pointing to 283° on the dial, which is 17° to the left of the approach course, giving a visual impression of wind drift to the left and therefore giving a possible reason for a heading correction to the right.
3) The navigator in a stressed and overloaded working situation most probably followed the rule setting the landing course 283° on the GPS in OBS mode instead of the approach course 300°.
4) The crew was not fully aware of the status of an AFIS officer in comparison with the authority of a Russian air traffic controller with the result that the crew accepted safety information from the AFIS officer as orders.
5) The crew had limited knowledge of the English language with the consequence that they had problems communicating their intentions to the AFIS officer.
6) The navigator was overloaded with tasks leaving little time for rechecking his work, thereby setting the scene for making mistakes.
7) The pilots did not monitor the work of the navigator sufficiently.
8) Leaving the communication with AFIS to the navigator during the approach was not according to the normative documents.
9) Due to the workload of the navigator, the decision of the co-pilot to transfer the responsibility of controlling the aircraft laterally to him, was inappropriate.
10) The crew resource management of the PIC was not satisfactory.
11) When the crew had made the decision to carry out the approach to runway 28, a new approach briefing was not accomplished.
12) The crew made the proper correction for the wind drift, but did not try to intercept the outbound track from ADV with the consequence that they overshot the approach centerline turning inbound.
13) Seemingly confusing indications on the HSIs in the base turn caused the crew to become uncertain of the aircraft position in relation to the LLZ 28 centerline. In this situation, the crew showed a lack of situational awareness.
14) The two pilots did not have the approach chart in front of them at all times during the approach making it difficult for them to maintain situational awareness.
15) The crew did not know of the possibility to check the position of the aircraft in relation to the localizer centerline by the VDF service available.
16) On final approach the crew probably put too much emphasis on the indications displayed on the GPS.
17) The crew started descent in a mountainous area without firm and positive control of the lateral navigation demonstrated by the disagreement within the crew as to whether to correct to the left or right.
18) In spite of the uncertainty within the crew as to whether they were approaching correctly or not, they continued instead of abandoning the approach and climbing to a safe altitude to solve the problem.
1) There is no Russian procedure for offset localizer approaches modifying the required rule to set the landing course on the HSI.
2) The course selected on both HSIs was 283° even though the approach course is 300°. This setting does not affect the indication of the CDI. However, the CDI was pointing to 283° on the dial, which is 17° to the left of the approach course, giving a visual impression of wind drift to the left and therefore giving a possible reason for a heading correction to the right.
3) The navigator in a stressed and overloaded working situation most probably followed the rule setting the landing course 283° on the GPS in OBS mode instead of the approach course 300°.
4) The crew was not fully aware of the status of an AFIS officer in comparison with the authority of a Russian air traffic controller with the result that the crew accepted safety information from the AFIS officer as orders.
5) The crew had limited knowledge of the English language with the consequence that they had problems communicating their intentions to the AFIS officer.
6) The navigator was overloaded with tasks leaving little time for rechecking his work, thereby setting the scene for making mistakes.
7) The pilots did not monitor the work of the navigator sufficiently.
8) Leaving the communication with AFIS to the navigator during the approach was not according to the normative documents.
9) Due to the workload of the navigator, the decision of the co-pilot to transfer the responsibility of controlling the aircraft laterally to him, was inappropriate.
10) The crew resource management of the PIC was not satisfactory.
11) When the crew had made the decision to carry out the approach to runway 28, a new approach briefing was not accomplished.
12) The crew made the proper correction for the wind drift, but did not try to intercept the outbound track from ADV with the consequence that they overshot the approach centerline turning inbound.
13) Seemingly confusing indications on the HSIs in the base turn caused the crew to become uncertain of the aircraft position in relation to the LLZ 28 centerline. In this situation, the crew showed a lack of situational awareness.
14) The two pilots did not have the approach chart in front of them at all times during the approach making it difficult for them to maintain situational awareness.
15) The crew did not know of the possibility to check the position of the aircraft in relation to the localizer centerline by the VDF service available.
16) On final approach the crew probably put too much emphasis on the indications displayed on the GPS.
17) The crew started descent in a mountainous area without firm and positive control of the lateral navigation demonstrated by the disagreement within the crew as to whether to correct to the left or right.
18) In spite of the uncertainty within the crew as to whether they were approaching correctly or not, they continued instead of abandoning the approach and climbing to a safe altitude to solve the problem.
Final Report:











