Crash of a Cessna 425 Conquest I in Helena
Date & Time:
Aug 11, 2021 at 0900 LT
Registration:
N783MB
Survivors:
Yes
Schedule:
Faribault - Missoula
MSN:
425-0103
YOM:
1982
Crew on board:
1
Crew fatalities:
Pax on board:
2
Pax fatalities:
Other fatalities:
Total fatalities:
0
Captain / Total hours on type:
800.00
Aircraft flight hours:
9576
Circumstances:
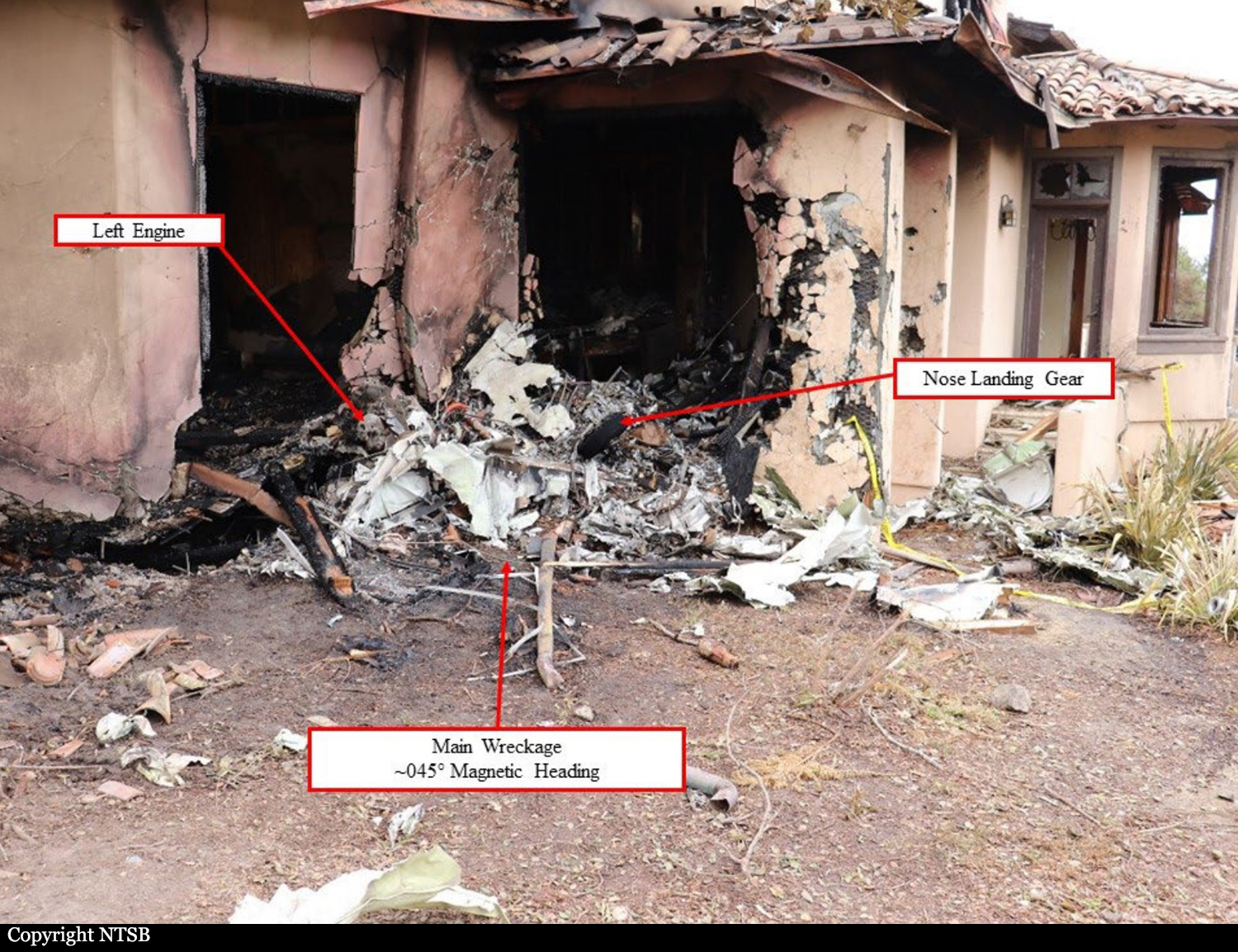
The pilot stated that on the morning of the accident he filled both wing fuel tanks to full. After takeoff, he climbed to his planned cruise altitude of 24,000 ft mean sea level (msl). While en route to his destination, the pilot reported that the left engine experienced a flame-out. The pilot opted to divert from the originally planned destination and descended. When the airplane was about 7,900 ft msl, the pilot reported that the right engine experienced a loss of power and that he was not going to be able to make it to the airport. Shortly thereafter, the airplane collided with trees and the airplane came to rest with the right wing and empennage severed from the fuselage.
Probable cause:
A flameout of both engines due to fuel starvation for reasons that could not be determined due to the airplane’s damage. There was fuel in the wing tanks at the time of the impact. Postaccident examination of the wreckage did not reveal any anomalies. A partial amount of fuel was found in both of the filter bowls, but it is unknown if fuel was able to reach the engines. A complete examination of the fuel system could not be completed due to the damage incurred to the airplane at impact. Both engines flaming out within a short time of one another is likely indicative of a fuel supply or delivery issue; however, the nature of the problem could not be identified during postaccident examination.
Final Report: